If you are setting up or updating an anatomy teaching program in Australia, you have probably weighed up the two dominant alternatives to traditional cadaveric dissection — plastinated specimens and 3D printed models. Both are marketed as modern, ethical, and effective. Both have genuine strengths. But they are fundamentally different tools, and choosing the wrong one for your context wastes money and compromises learning outcomes.
What Is Plastination?
Plastination is a preservation technique developed by Gunther von Hagens in 1977. Real human (or animal) tissue is treated to replace water and fat with curable polymers — typically silicone, epoxy, or polyester resin. The result is a dry, odourless, durable specimen that retains the exact anatomical structure of the original tissue.
Because they start with real human remains, plastinated specimens carry an inherent authenticity that manufactured models cannot replicate. The tissue architecture, surface textures, and spatial relationships are real — not approximated.
What Are 3D Printed Anatomy Models?
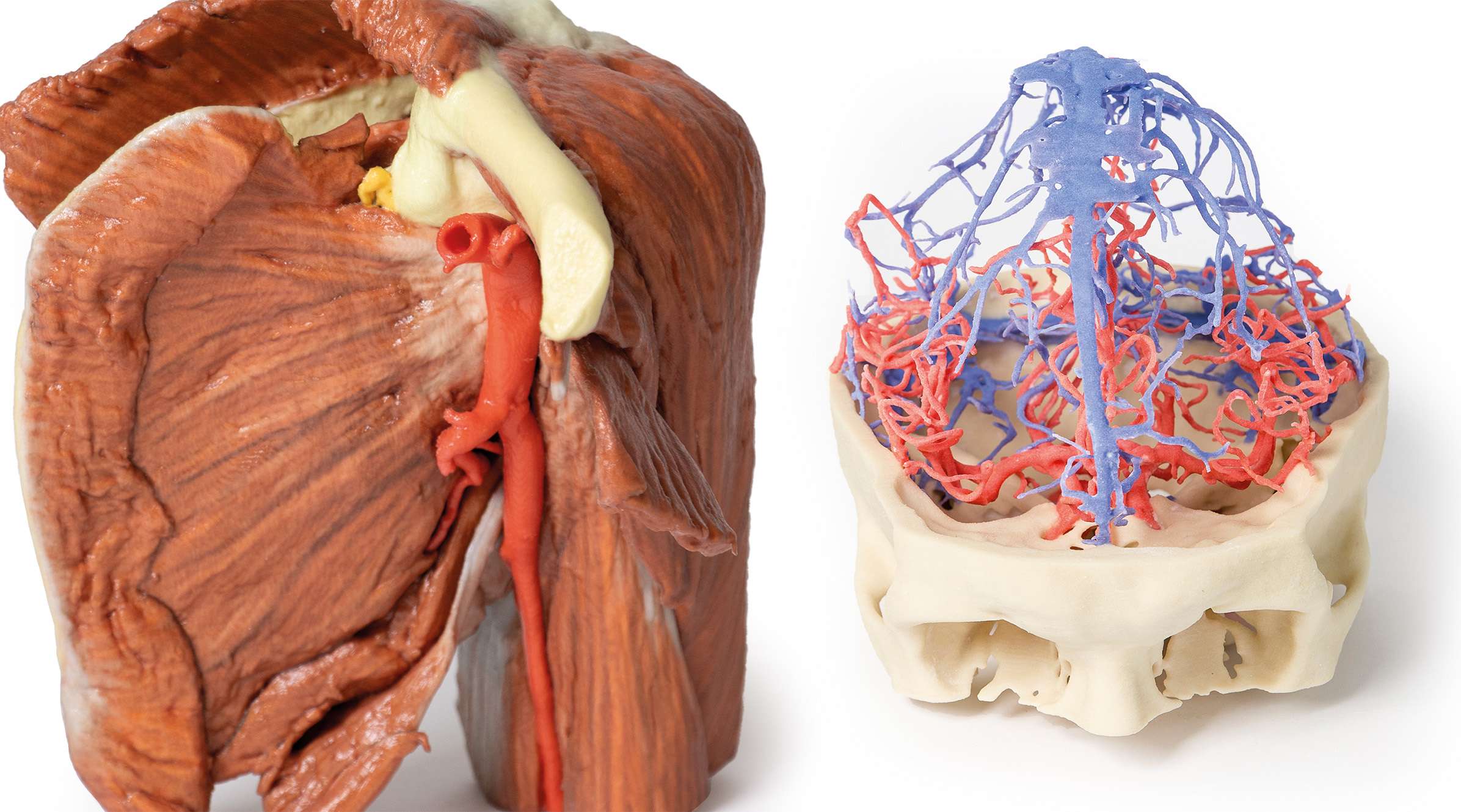
3D printed anatomy models are manufactured from digital imaging data — typically CT or MRI scans of real patients. The scan data is segmented, cleaned, and printed using medical-grade polymers in multiple colours and materials to represent different anatomical structures.
They are not derived from human tissue. They are engineered reproductions of real anatomy, accurate to the resolution of the original scan data.
Head-to-Head Comparison
Anatomical Realism
Plastinated specimens win here. Because they are real tissue, they preserve micro-architecture, fascial planes, and tissue relationships that no manufacturing process can fully replicate. Students handling a plastinated heart are touching the actual cardiac muscle, valve leaflets, and coronary vessels of a real person.
3D printed models are anatomically accurate at a macro level — the shape, size, and spatial relationships are faithful to the source scan — but they cannot reproduce tissue texture, elasticity, or the subtle layering of fascia and connective tissue.
Pathology Teaching
3D printed models have the edge. Because they are manufactured from scan data, you can build a library of specific pathologies — a Type A aortic dissection, a Wilms tumour, a hemisected brain with a glioblastoma — and reproduce them indefinitely. If a model breaks or wears out, you print another one.
Plastinated pathology specimens exist, but they depend on sourcing donors with the specific pathology you need. You cannot order a plastinated Berry aneurysm the way you can order a 3D printed one.
Ethical and Regulatory Considerations
3D printed models are simpler. They involve no human tissue, no donor consent requirements, no biological hazard protocols, and no cultural sensitivities around the handling of human remains. For institutions that serve diverse student populations — including those with religious or cultural objections to handling cadaveric material — 3D prints remove a significant barrier to participation.
Plastinated specimens require sourcing through body donation programs, which are subject to strict ethical oversight and consent frameworks. The legal and regulatory environment in Australia (governed by state-based anatomy acts) adds complexity.
Durability and Maintenance
Both are excellent. Plastinated specimens are dry and stable at room temperature — no formalin, no refrigeration, no biological waste. 3D printed models are similarly inert and shelf-stable. Both can last decades with reasonable care. The difference is that a damaged 3D print can be replaced from the same file. A damaged plastinated specimen is irreplaceable.
Cost
3D printed models are generally cheaper on a per-unit basis, especially for common structures. Plastination is labour-intensive and time-consuming (weeks to months per specimen), which drives higher unit costs. However, a plastinated full-body prosection provides breadth that would require dozens of individual 3D prints to match.
Student Learning Outcomes
Published research (including studies from BMC Medical Education and Anatomical Sciences Education) consistently shows that objective test scores are comparable between students using plastinated specimens and those using 3D printed models. Students subjectively rate plastinated specimens as more "realistic" and emotionally impactful, while they rate 3D prints as easier to use, clearer to interpret, and more practical for self-directed study.
So Which Should You Choose?
The honest answer is that it depends on what you are teaching and who you are teaching.
- For undergraduate anatomy courses where the goal is spatial understanding and identification of structures — 3D printed models offer excellent value, clarity, and scalability.
- For postgraduate surgical or clinical anatomy where tissue handling, dissection skills, and real-tissue appreciation matter — plastinated specimens (or cadaveric work) remain the gold standard.
- For pathology teaching at any level — 3D printed models are the clear winner due to the breadth and reproducibility of the catalogue.
- For institutions with cultural diversity or ethical constraints — 3D printed models avoid the complexities of human tissue handling entirely.
Many of the best anatomy programs in Australia use both, deploying each tool where it adds the most value.
What We Supply
We carry a full range of 3D printed anatomy and pathology specimens created from real patient scan data. For institutions looking to compare options or build a mixed teaching collection, get in touch — we can advise on the best combination for your curriculum and budget.